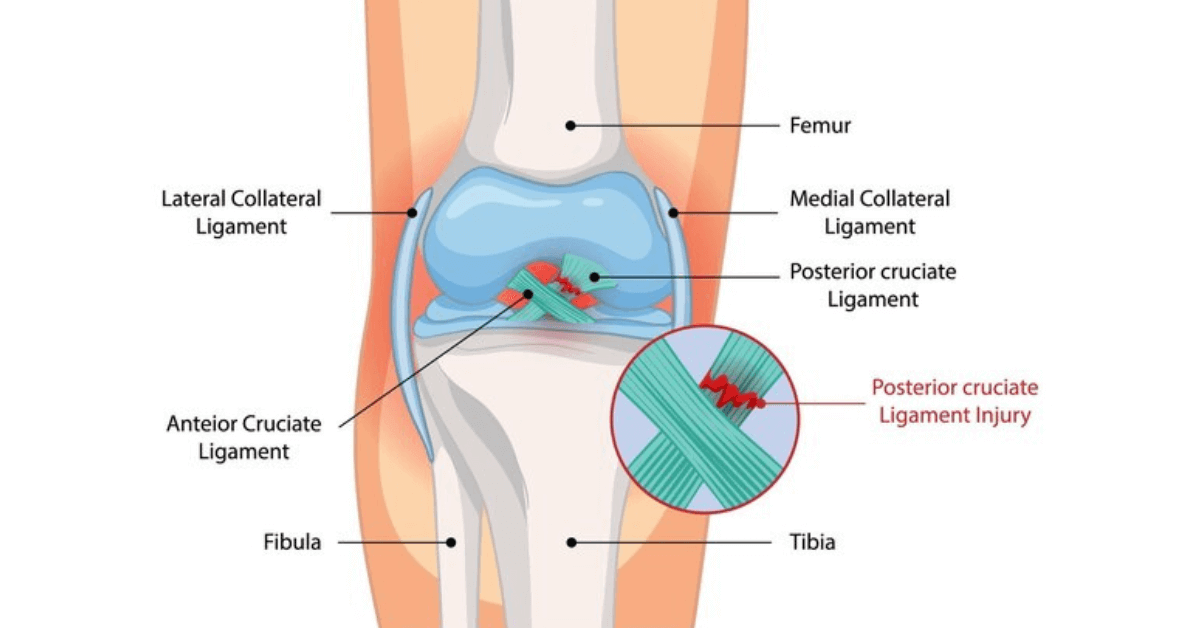
What Is PCL Reconstruction?
PCL reconstruction repairs or replaces the torn posterior cruciate ligament using autograft or allograft tissue. Navigated tunnels and internal bracing restore the tibia’s position beneath the femur, eliminating posterior sag, improving stair descent, and protecting cartilage from abnormal loading.
PCL Surgical Techniques
- Single-bundle reconstruction: Recreates the anterolateral bundle for most isolated Grade III tears.
- Double-bundle reconstruction: Restores both bundles in high-demand athletes or complex laxity.
- Internal brace augmentation: High-strength suture tape protects the graft during early healing.
- Combined ligament repair: Address MCL, LCL, or posterolateral corner injuries in the same sitting.
When Is PCL Reconstruction Needed?
Surgery is recommended when instability interferes with daily life or when associated ligaments are injured alongside the PCL.
- Grade III tears: Posterior sag greater than 10 mm on stress radiographs.
- Multi-ligament injuries: Knee dislocations, sports trauma, or road accidents with combined damage.
- Chronic instability: Difficulty descending stairs, kneeling, or carrying loads due to giving way.
- Revision cases: Failed conservative treatment or previous surgery with persistent laxity.
Telos stress X-rays, MRI, and dynamic ultrasound help quantify laxity and visualise associated structures before surgery.
PCL Reconstruction Steps
Restoring posterior stability demands precision and protection of neurovascular structures.
- Patient positioning: Special supports and fluoroscopy visualise tunnel trajectory safely.
- Posterior arthroscopy: Allows assessment of meniscus root or cartilage lesions.
- Tunnel creation: Guides protect the popliteal artery while drilling the tibial tunnel.
- Graft fixation: Suspensory buttons, interference screws, and internal brace tape secure the reconstruction under fluoroscopic confirmation.
Benefits of Modern PCL Surgery
- Restored stability: Eliminates posterior sag and improves confidence on stairs.
- Protected cartilage: Balanced tibiofemoral contact reduces long-term arthritis risk.
- Enhanced athletic performance: Athletes regain power for sprinting, jumping, and cutting.
- Comprehensive care: Associated ligament and meniscus injuries are addressed simultaneously.
Rehab Milestones
- Weeks 0–2: Hinged brace locked in extension, quad activation, and swelling control.
- Weeks 3–6: Gradual flexion to 90°, closed-chain strengthening, and gait training with crutches.
- Months 3–4: Dynamic balance, step-down drills, and cycling once quadriceps strength improves.
- Months 6–8: Sport-specific drills, plyometrics, and posterior chain strengthening.
- Clearance testing: Objective strength and motion assessments before return to competition.
Risks & Safeguards
PCL reconstruction requires specialist expertise; our protocols reduce complications significantly.
- Neurovascular injury: Avoided with posterior portals, fluoroscopy, and experienced surgeons.
- Postoperative stiffness: Managed with early controlled motion and dedicated physiotherapy.
- Residual laxity: Minimized via accurate tunnel placement, double-bundle techniques, and internal bracing.
- Blood clots: Prophylaxis includes compression devices, medication, and early mobilisation.
- Graft stretch-out: Patient education emphasises brace compliance and gradual loading.
With advanced imaging, precise instrumentation, and specialised rehab, Joint Robo delivers predictable posterior knee stability.