What Is MCL Treatment?
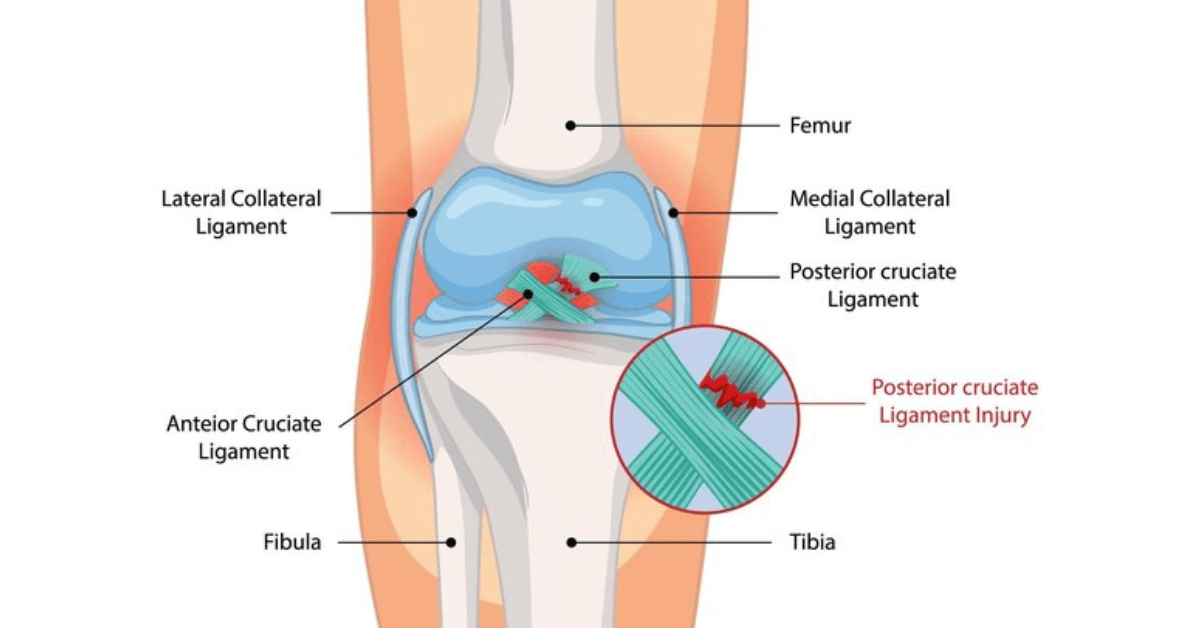
The medial collateral ligament stabilises the inner knee against valgus forces. Mild injuries heal with bracing and targeted rehab, while high-grade tears or chronic laxity may need surgical repair, augmentation, or reconstruction using tendon grafts and internal braces to restore stability.
MCL Treatment Spectrum
- Functional bracing: Hinged braces protect healing fibres during early phases.
- Ultrasound-guided injections: PRP or prolotherapy accelerates healing in partial tears.
- Primary repair: Acute avulsions are reattached to bone with anchors.
- Anatomic reconstruction: Tendon grafts recreate superficial and deep bundles for chronic laxity.
When Do We Recommend Surgery?
Most Grade I–II injuries respond to conservative care, but certain scenarios demand operative intervention.
- Grade III tears: Complete disruption with >10 mm valgus opening on stress tests.
- Knee dislocations: Multi-ligament injuries that require comprehensive reconstruction.
- Chronic instability: Persistent valgus laxity impairing sport or daily activities.
- Failed non-operative care: Pain or giving way despite bracing and physiotherapy.
Stress ultrasound, MRI, and dynamic fluoroscopy quantify damage and guide personalised treatment decisions.
MCL Repair & Reconstruction Steps
Surgical care focuses on restoring native anatomy while protecting surrounding structures.
- Diagnostic arthroscopy: Evaluates meniscus and cruciate integrity, addresses concurrent lesions.
- Anatomic landmarking: Fluoroscopy or navigation marks femoral and tibial footprints.
- Graft preparation: Hamstring or allograft tendons are sized to match required length.
- Fixation: Interference screws and internal brace tape secure the graft while maintaining isometry through flexion.
Benefits of Comprehensive MCL Care
- Stable valgus control: Prevents knee from “caving in” during cutting or squatting.
- Meniscus protection: Restored alignment protects medial meniscus from overload.
- Faster return to play: Structured progression rebuilds confidence for sport.
- Lower reinjury risk: Internal bracing and neuromuscular training guard against relapse.
Rehab Roadmap
- Weeks 0–2: Hinged brace locked, quad activation, and swelling control.
- Weeks 3–6: Gradual flexion, closed-chain strengthening, and balance drills.
- Months 3–4: Sport-specific drills, lateral movement training, and proprioception work.
- Month 6: Return-to-play testing with single-leg hop and strength symmetry benchmarks.
- Ongoing: Maintenance programmes to sustain medial chain strength.
Risks & Precautions
MCL treatment is safe, yet vigilance ensures optimal outcomes.
- Residual laxity: Prevented with accurate graft placement and postoperative bracing.
- Stiffness: Early physiotherapy and motion limits tailored to graft tension avoid arthrofibrosis.
- Infection: Rare due to minimally invasive techniques and perioperative antibiotics.
- Nerve irritation: Saphenous nerve branches are protected with careful dissection.
- Recurrent injury: Neuromuscular retraining and return-to-play testing reduce recurrence.
Regular follow-ups, motion analysis, and strength assessments keep your knee resilient long after treatment.